The same device that is driving you crazy could hold the keys to solving our mental health crisis.
Early in her career, when she was a junior researcher building artificial intelligence systems at the MIT Media Lab, Rosalind Picard was unsure what to do with data she encountered on the impact of emotions on human perception and cognition. The findings were compelling — but they also made her uneasy.
Bringing up the “e-word” as a serious research topic, she says, was “a great way to end your career” — and she was trying to get tenure, Picard told me. “I kept bumping into all these roles emotion was playing and trying to figure out how to fit that into my mathematical models of the brain. And I did not want to jump into that because I was a woman in science.”
Nevertheless, she persisted, writing a “thought piece” that she circulated among colleagues at the Media Lab, arguing that building truly intelligent machines required insights about the role of emotions and feelings. She eventually submitted these ideas to a journal and got a prompt rejection. “One of the reviews,” she wrote recently, “indicated that the content was better suited to an in-flight magazine.”
She was lucky in one way, she says: The Media Lab was “probably the only place where the more loony and ridiculous and crazy your ideas are, the more they liked you.” She ended up shaping her ideas into a book whose title, Affective Computing, gave a name to a whole new field that she essentially invented. She also got tenure.
Now Picard, who heads a program on affective computing at the Media Lab, is at the forefront of a radical new idea: that your emotional state can be objectively measured using wearable devices or by tracking patterns in the way you type and talk on your mobile phone. Emotions and feelings — once seen as fuzzy and ill-defined — have physical correlates that can be measured and described, she says. The resulting data can help predict whether a person is becoming depressed or anxious, experiencing other mental challenges — or starting to improve.
“I’ve always found emotion like weather,” Picard says. “You can measure the rainfall, you can measure the barometric pressure, you can measure the temperature and humidity. Every now and then, a particular set gets a special name like a hurricane, much like you can have a special state called anger or depression. But underneath the anger or the depression are lots of continuously changing things in our body that change with stress, with social change, with physical activity, with novelty, with what you eat and how you sleep. As we start to make it easy for those things to be measured, we start to make it possible to build the equivalent of meteorological models that forecast the weather.”
But while you can’t change the weather, it might be possible to change your emotional forecast. Picard is working on a system that will send people alerts about moods that are on the way, like a gathering storm — along with suggestions for ways to intervene.
“I’ll glance at my phone and it says: ‘40 percent chance your stress is going to be higher, 20 percent chance you’re going to be sick, 40 percent chance your mood is going to drop,’” Picard says. “We also hope to give data-driven recommendations of things they might consider doing if they want to change the weather forecast: ‘Go to bed two hours early. Get some sunshine and an hour of walking. Reach out to one of these friends who usually cheers you up.’”
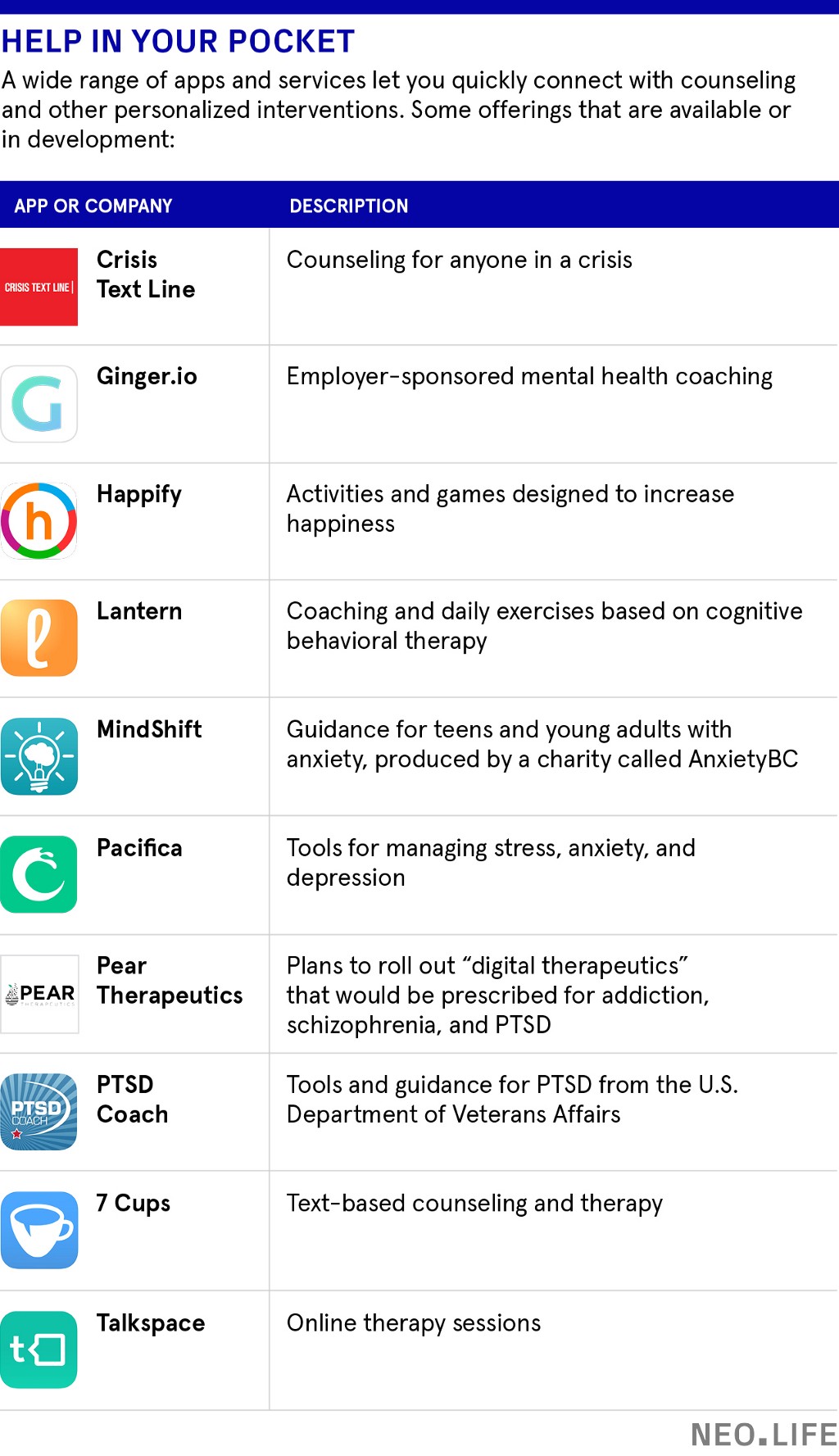
Picard makes a bold claim about the potential of the technology: she thinks most of the depression that people experience can eventually be prevented. But she’s not alone in hoping to use mobile devices to improve mental health, from apps that offer real-time counseling to “digital therapeutics” that will eventually be prescribed for people suffering from a range of conditions.
Yes, the very devices that are creating new forms of addiction and stress can instead deliver therapy or provide support. Mobile phones may be part of the problem, Picard says, but they also can be part of the solution.
Bending the curve
That Picard, a computer engineer, would place faith in a technological solution is hardly unusual. What’s more surprising is that a mainstream mental health and neuroscience researcher like Thomas Insel also sees the potential in using cell phones to improve mental health. Insel ran the National Institute of Mental Health, the world’s largest funder of research on mental disorders and treatment, for 13 years. He left in 2015 to take charge of mental health initiatives at Google’s life science subsidiary, Verily, and then left after 18 months to join a startup, Mindstrong Health, as co-founder and president. Mindstrong has raised $14 million on the idea that health care systems can use their patients’ phones to learn more about their condition and provide better diagnosis and treatment.
“A lot of our lives are played out on these little computers we all have,” Insel says. “If you’re trying to understand someone’s mental state, their behavioral state, it’s not a crazy idea that a lot of who they are at that moment in time is going to be represented on the phone.”
Mindstrong has forged partnerships with health-care providers and academic researchers to study thousands of patients, each carrying cell phones outfitted with Mindstrong’s app. The app will allow researchers to use the phone’s microphones, keyboards, and location functionality to measure how quickly people respond to text messages, how fast or slow they type, the force with which they hit the keys, and their patterns of late-night texting and browsing.
The researchers will also be able to see the individual words people send in text messages — but not groups of words or phrases. “If you type, ‘I love you,’ we will have ‘I’ and ‘love’ and ‘you’ in some pool of thousands and thousands of words,” Insel says. “If you type ‘love’ 16 times a day, I’ll know that, but I won’t know it was connected to I and you” — or even preceded by the word “don’t.” The team will refrain from gathering strings of words, he says, because “it’s creepy for someone to be looking at your email or your text messages.” Similarly, he says, they won’t use the phone’s microphone or camera to analyze the way people speak or look because users are likely to find this invasive.
Insel speaks softly and calmly, but his message is at once urgent and implicitly self-critical. The mental health research establishment he led has done little to change the trajectory of mental illness in America. The PowerPoint slides from the talks he gives around the country make the point.
“My hope is that in the future there will be 80 percent less depression, that most cases will be prevented.”
“U.S. suicide rate unchanged in 2 decades” says one slide, over a graph that shows suicides hovering just north of 12 per 100,000 in 1990 and in 2010. “Mental Disorders Top The List Of The Most Costly Conditions In The United State: $210 Billion,” says another. “Why have we failed to bend the curve?”
There are many answers to that question, Insel says. Diagnosis of mental disorders is ineffective and inconsistent, with clinicians using symptom checklists that resemble multiple-choice menus. Most people who need treatment aren’t getting it. And when treatment is provided, little is done to measure whether it’s actually working.
If used wisely, Insel argues, cell phones can address many of these issues.
Mindstrong wants to develop a system that health care providers — OptumHealth has signed on as one partner — would use as part of a more holistic approach to patients. The signals that emerge from tracking patients’ cell-phone behavior would flow to “care managers” — medical assistants who are the first point of contact with a patient and work closely with their primary care doctor, as well as with their therapists and psychiatrists. They may visit patients at home and reach out to their families.
“It’s actually not a high-tech solution,” Insel says. “The tech part is providing that care manager with a dashboard of information so that he or she knows who’s starting to [deteriorate], or who’s doing well. Right now they don’t have a lot of information. They often find out somebody is not doing well when they show up in the E.R. We’ve got to do better than that. … You want to catch all of this before it becomes a crisis.”
Insel has seen up close how one revolution after another in psychology created excitement but ultimately failed to reduce the devastating incidence and burden of mental illness. Ever the guarded researcher, he is both excited and cautious about the potential of this new approach. “Psychoanalysis was going to solve the problem, drugs were going to solve the problem, and then it was cognitive behavioral therapy,” he tells me over lunch at a Mexican restaurant in Oakland, California. “I think apps are extremely interesting and will solve certain problems. All these have something to contribute, but there is no magic bullet.”
Detecting extroverts
In addition to smart phones, Picard’s group at the Media Lab adds another tool: wristbands with built-in sensors that can measure temperature, physical activity, and skin conductance — the strength of electrical signals in the skin. (When a person experiences emotional and physiological arousal, the skin better conducts electricity and these signals increase. Empatica, a company that Picard co-founded, sells these same wristbands to people with epilepsy, to alert them and their family to the onset of a seizure.)
In 2013, Picard’s group began the Snapshot study, which tracks MIT undergraduates using smartphone apps and the wristbands to gather a variety of data and correlate it with other measures of mental and emotional status. “When do they tend to be on the phone?” Picard asks, ticking off some of the metrics. “When do they tend to sleep? Are they stuck in the same place every day or getting out and about? What’s their rhythm over the week, on weeknights vs. weekends?”
The patterns found by Picard’s team don’t always predict the same outcomes, however. In one group of MIT students, sending a lot of text messages and having social interactions before bedtime generally correlated with their being in a good mood the next day. To Picard’s surprise, the exact opposite was true of another group: If they did a lot of texting and were social before bed, they seemed unhappier the next day.
“It was like we found the extroversion cluster and the introversion cluster,” Picard says. “There is just wonderful variety in people. One-size-fits-all advice is definitely going to become a relic of the past once we get a lot more data.”
Insel questions how effective a system will be if it requires people to wear a device in addition to the smartphone they carry. “MIT undergraduates will wear them (for a study), and tech people in Silicon Valley will wear four watches and look at them every day,” he says. “But in the real world, people don’t use wearables.”
But they sure do use their phones and apps. A company called 7 Cups is drawing 1.9 million monthly users, mostly millennials, in 189 countries, to its phone app, which provides free emotional and psychological support — via text — to anyone who wants it from a group of “listeners” — volunteers trained as peer counselors. Users who want professional help can pay to exchange text messages with licensed therapists.
“I think there’s a lot of emotional pain out there. A lot of people are struggling and there’s not a lot of ways for them to get help,” says Glen Moriarty, the psychologist who founded the company. “We provide an easy way.”
For Picard, these new models point toward a more hopeful future. As a mother of three and a college professor, she’s heartbroken by the levels of stress and depression she sees around her.
“We’ve got to wake up and start saying, ‘What have we been doing in the world that’s causing everything to get so much worse?’” she says. “We’re building technology that may be contributing. I feel a responsibility. My hope — and we’ll get there when we get enough data — is that in the future there will be 80 percent less depression, that most cases will be prevented. Health care will be about protecting health instead of about waiting until they’re so bad off that you get a diagnosis and enter the disease care system and they start trying to fix you. I think it’s going to be much more about prevention and keeping yourself strong and resilient.”






















